Distal Femur Fracture
What is it?
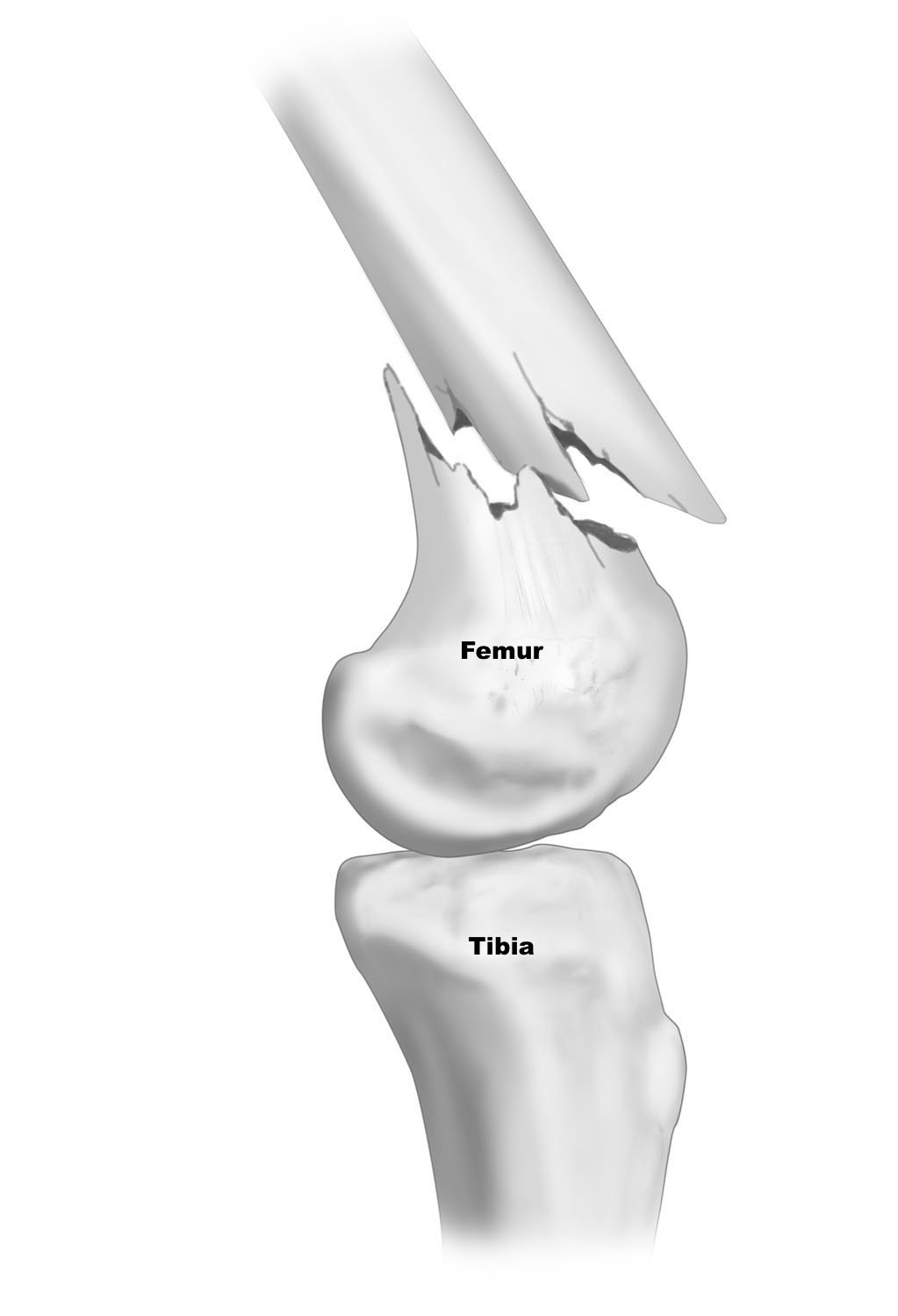
A Distal Femoral Fracture is a fracture found at the end of the thighbone(the distal femur). Distal femur fractures vary. The bone can break straight across (transverse fracture) or into many pieces (comminuted fracture). Sometimes these fractures extend into the knee joint and separate the surface of the bone into a few (or many) parts. These types of fractures are called intra-articular because they damage the cartilage surface of the bone. Intra-articular fractures can be more difficult to treat.
How does it get hurt/damaged?
Distal Femur Fractures occur primarily in two patient types, these being younger and older patients.
Injuries in the former, younger patients, most often happen due to a high energy collision such as a car crash or a sports injury. Due to the high level of force in these situations, patients may also experience other types of injuries alongside the fracture.
Olde patients most commonly experience a distal femur fracture from low force events. As we get older, our bones get thinner and become weaker. A low force event can cause an injury in someone who has weaker bones.
How common is a Distal Femur fracture?
Pretty common! Approximately 58,600 people experience a Distal Femur Fracture per year in the USA.
When should you be worried about a Distal Femur Fracture and what to do initially?
Distal Femur Fractures will require an immediate trip to your local emergency room. Once there, an emergency care provider will diagnose the severity of the injury and the treatment path. Often, these injuries can be significantly displaced meaning the fracture is causing the bone to be misaligned and possibly shortened, in which case it may be urgently necessary to replace the bone back in its normal position.
Severity of Injury and Treatment options?
Distal Femur Fractures vary in degree of severity. In general, fractures of the distal femur that are displaced-meaning the fracture is causing the bone to be misaligned- need surgery. These procedures are often complicated and require precision to restore the overall alignment of both the femur and the joint surfaces.
If it is a displaced fracture, then fracture fixation, like inserting a rod into the end of the femur to hold it in place or plates and screws on the side of the femur.
For a fracture that enters the joint space, if there is any significant disruption of the cartilage surface, surgery to restore the normal congruity of the joint surface may be needed.
A Hoffa fracture, which only involves one of the femoral condyles, can be difficult to treat because the fracture can be entirely through the cartilage surface, and the screws and other devices required to fix the fracture have to go into the cartilage to hold it in place.
Post-surgery, it is essential to enter into a rehabilitation program that emphasizes early motion. If the knee cannot be moved because the fracture is fragile, then there may be a risk of having the knee joint become stiff afterwards.
What is my recovery timeline and the anticipated outcome?
Most patients will need to be on crutches with minimal to no weight bearing for the first 6 weeks. Depending on the severity of the injury and the amount of hardware required to help reset the bone, a patient can usually expect to start bearing weight after the 6 weeks mark. Driving is usually allowed after 7 to 8 weeks, whereas the full recovery process can take longer, up to 4-6 more months.