Meniscus Tear
What is it?
A meniscus tear occurs in the rubbery knee cartilage that cushions the shinbone from the thighbone.
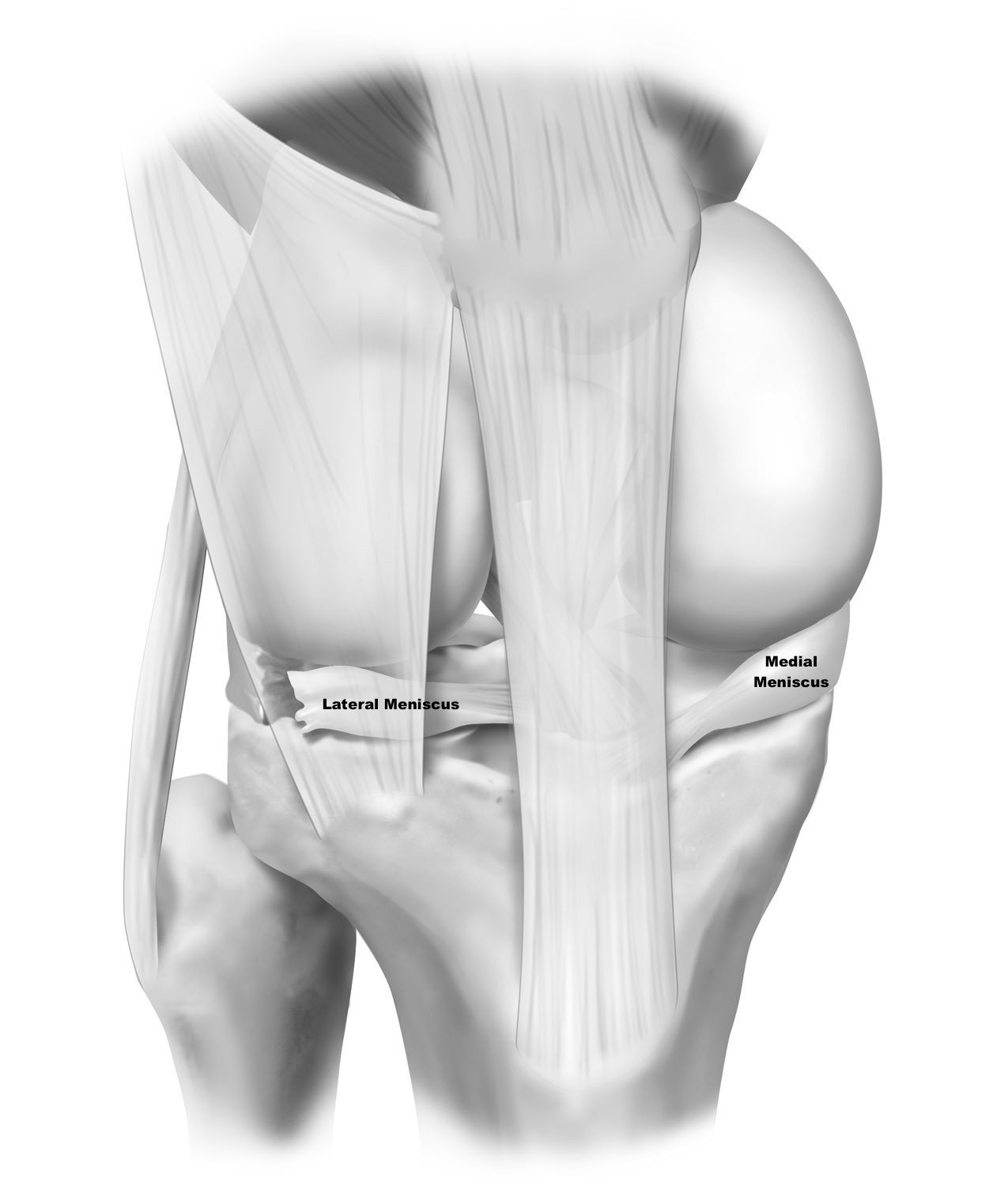
The meniscus is a C-shaped cushion that sits on both the inside (medial) and the outside (lateral) part of the knee. It essentially acts as the shock absorber of the knee. Due to its tough and rubbery texture, the meniscus is able to translate and control the amount of energy that the tibia receives through every step, and especially when you land from a jump or when lifting weights. The meniscal structures have three zones that make up the C-shape: a front part called the anterior horn, the middle portion called the body, and a portion in the back, the posterior horn. All three of these parts are attached to the tibia by the meniscal roots, which keep the meniscus from moving out of place during knee motion.
How does it get hurt/damaged?
Injury to the meniscus can happen a few different ways, including but not limited to twisting, turning, or pivoting type activities. This injury commonly happens in athletes who participate in sports with a high chance of pivoting like football, basketball, or soccer. A tear can also occur due to hyper flexion of the knee, caused by a deep squat or lifting.
How common is a meniscus tear?
Meniscus tears happen in 61 out of every 100,000 people (0.061% of the population) and more often seen in individuals who are physically more active.
When should you be worried about a meniscus tear and what should you do initially?
Meniscus tears that happen in isolation aren’t necessarily an emergency level concern. However, if you have any intractable pain, locking or any other concerning sign or symptoms, you should schedule an appointment with your primary care provider or go to the emergency room.
What is the severity of the injury and the treatment options?
Meniscus tear severity is usually graded according to its appearance on an MRI scan. Grade 1 and 2 intrasubstance meniscus tears are only within the body of the meniscus on MRI scans and cannot be seen at the surface during an arthroscopy. Usually these can be treated without surgery. Grade 3 tears are tears that extend all the way to the surface and have little to no connection to the tibia.
Treatment options depend on the varying severity of the tear. If a patient has a reparable meniscus tear, and they’re young or have very little arthritis, it’s best to have the meniscus repaired, if possible. The most common technique is the all-inside technique where the surgeon sutures the meniscus without having to make incisions. The inside-out technique places meniscus sutures from inside the joint to outside the joint and catches the needles through an incision on the medial or lateral aspect of the joint. The other, but less common, technique is to make a small incision in the front of the knee and place sutures from the outside of the knee to inside of the knee.
With the very different types of tears, a number of them are degenerative type tears that can cause pain when they catch in the joint or when you squat, twist, turn, or pivot. In the types of tears, if they are located closer to the middle of the knee, there may not be enough meniscus tissue present to have the opportunity for a repair. In these circumstances, a patient should have the meniscus trimmed, or have the torn portion of the meniscus is removed. The reason most meniscal tears are trimmed and taken out is because the meniscus itself doesn’t have an abundant blood supply, especially on the inner parts of the meniscus.
Whatever meniscus volume remains after trimming is essential to slow down any rate of arthritis. Therefore, if it’s possible, you should have a non-repairable meniscus trimmed in a technique called saucerization. In this technique, the edges of the meniscus that probably will not tear further could still act as a cushion if needed.
A special type of meniscus tears is meniscal root tears, where the meniscus gets detached from the bone and floats around the knee. This is almost the equivalent to not having a meniscus, requiring immediate attention.
Meniscus tears that are non-displaced, or causing minimal pain, in older patients may be treated with a program of physical therapy and observation. Bucket handle, meniscal root tears, and radial tears of the meniscus, especially in younger patients, usually need surgery sooner rather than later. In general, if the meniscus is reparable and the patient is younger, surgery is recommended to try to preserve the meniscus function. For tears that are not reparable, a trial of physical therapy can be attempted.
What is my recovery timeline and the anticipated outcome?
Meniscus tears vary in recovery timeline, where patients who have a meniscus repair may take longer to recover, but often can get to full activities with a better long term prognosis. Patients who have a meniscus removed often return to activities much quicker but then will start to develop arthritis and have to decrease activities over time. The takeaway should be that even though it is easier to have your meniscus taken out right away, the long term benefits and overall quality of life might not be as high as one would like.
Patients who do have a meniscectomy will be on crutches for 2-7 days and will return to activity in 4-6 weeks. Patients who have a meniscus repair will need to be non-weightbearing on crutches for the first 6 weeks and then can slowly wean off the use of crutches when they can walk without a limp. General return to full activity will be around 5-8 months.